Modern Coal Miners Have Higher Death Rates From Lung Diseases Than Their Predecessors
Posted on by
Coal mine dust causes a range of lung diseases, collectively called coal mine dust lung diseases. Examples include coal workers’ pneumoconiosis (CWP, a dust-induced scarring lung disease commonly called black lung), chronic obstructive pulmonary disease (COPD), and lung function impairment. All of these cause substantial morbidity (illness) and mortality (death) among affected coal miners.[1–5] Most attention in the U.S. has focused on CWP, especially its most severe stage called progressive massive fibrosis. [6–8] Unfortunately, this has overshadowed the burden of other diseases that occur in coal miners.
New research finds that coal miners are also at increased risk of death from other diseases, including COPD and lung cancer. Controlling exposures to respirable coal mine dust can help prevent these serious diseases.
What We Did
Researchers at the University of Illinois Chicago and NIOSH recently published the largest existing study on causes of mortality in U.S. coal miners.
We analyzed cause of death data from the National Death Index on 235,550 U.S. coal miners who died between 1979 and 2017 and had participated in either the NIOSH Coal Workers’ Health Surveillance Program or the Department of Labor’s Federal Black Lung Program. We compared the odds of death from specific causes in our population of coal miners to the odds of death from the same causes in the general non-Hispanic white, male U.S. population. Miners were divided into four groups: those born before 1920, between 1920 and 1929, between 1930 and 1939, and after 1940.
What We Found
We found that coal miners have significantly increased odds of death from CWP, COPD, and lung cancer compared with their counterparts in the U.S. population. This higher mortality has also worsened over time with modern miners facing greater risk than their predecessors. Miners in the Central Appalachian states of Kentucky, Virginia, and West Virginia face the most severe risk. Central Appalachian coal miners born in 1940 or later had over eight times the odds of dying from a nonmalignant respiratory disease such as black lung or COPD than their counterparts in the general population (See Figure 1). This eight-fold increase was the highest odds of death from nonmalignant respiratory disease in all the age groups examined. Progressive massive fibrosis, which is only caused by dust inhalation, was also more frequent in younger age groups. Thus, it appears likely that coal mine dust inhalation also contributed to their increased burden of nonmalignant respiratory disease.
Figure 1. Mortality odds ratios from nonmalignant respiratory disease among coal miners compared to non-coal miners in Central Appalachia. Population restricted to those aged 45 and older at time of death.
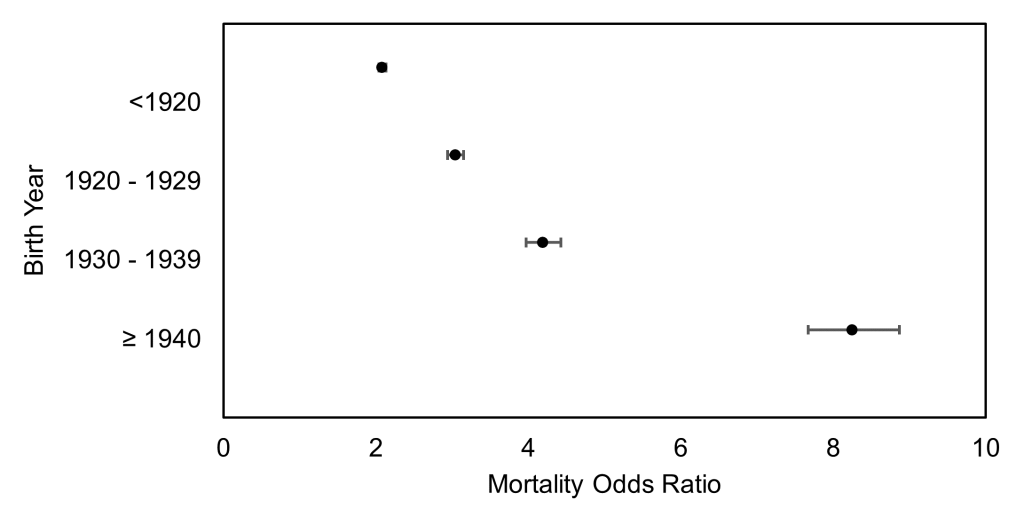
Nonmalignant respiratory diseases include pneumoconioses (CWP and silicosis) and other chronic lower respiratory diseases that can be caused by coal mine dust such as COPD. While younger cohorts had higher odds of death compared to older cohorts, all mining cohorts had consistently and significantly elevated odds of death from chronic lower respiratory diseases, the majority from COPD, among coal miners compared with the general population of U.S. males. This was true across every birth cohort and in nearly every age group nationally and within Central Appalachia. These findings underscore the importance of preventing chronic lower respiratory diseases like COPD caused by respirable coal mine dust and other factors in coal miners.
In addition to the nonmalignant lung diseases discussed above, coal miners face potential exposure to known carcinogens in their work environment including diesel exhaust, silica, asbestos, and radon. Nationally, we found across all four birth cohorts that coal miners had significantly increased odds of death from lung cancer compared with the general U.S. population. Our findings add to the growing literature that coal miners are at risk of increased mortality from lung cancer. Controlling exposure to respirable crystalline silica is an important aspect of prevention. A recent study of regulatory dust monitoring data from 1980 to 2017 revealed that the percentage of silica-containing respirable dust was significantly higher in Central Appalachian underground mines compared with those in the rest of the U.S. suggesting the greatest potential for exposure in this region.9 Increased lung cancer mortality in coal miners also suggests the importance of offering eligible coal miners the opportunity to have lung cancer screening using low-dose CT scan so cancer can be detected at early stages when treatment has the best outcome.
We observed significantly lower odds of mortality from ischemic heart disease among Central Appalachian coal miners compared with their white male counterparts in the general population, consistent with other studies. This might be because miners performing strenuous work in coal mines have better cardiovascular fitness than the general population, the so-called healthy worker effect.
Recent scientific and media attention has been focused on rising rates of pneumoconiosis in coal miners, which is only one of the diseases caused by coal mine dust. This study shows that U.S. coal miners are also at increased risk for other diseases, including COPD and lung cancer. Prevention efforts that include controlling exposures to respirable coal mine dust should address all of these serious diseases.
Kirsten Almberg, PhD, is an occupational epidemiologist with the University of Illinois Chicago School of Public Health, Environmental and Occupational Health Sciences Division and a guest researcher in the Respiratory Health Division, National Institute for Occupational Safety and Health.
Robert Cohen, MD, is an occupational pulmonologist with the University of Illinois Chicago School of Public Health, Environmental and Occupational Health Sciences Division and a Senior Consultant to the Respiratory Health Division, National Institute for Occupational Safety and Health.
References
- Attfield MD, Kuempel ED. Mortality among U.S. underground coal miners: a 23-year follow-up. Am J Ind Med. 2008;51(4):231-245. doi:10.1002/ajim.20560
- Graber JM, Stayner LT, Cohen RA, Conroy LM, Attfield MD. Respiratory disease mortality among US coal miners; results after 37 years of follow-up. Occup Environ Med. 2014;71(1):30-39. doi:10.1136/oemed-2013-101597
- Miller BG, MacCalman L. Cause-specific mortality in British coal workers and exposure to respirable dust and quartz. Occup Environ Med. 2010;67(4):270-276. doi:10.1136/oem.2009.046151
- Une H, Esaki H, Osajima K, Ikui H, Kodama K, Hatada K. A prospective study on mortality among Japanese coal miners. Ind Health. 1995;33(2):67-76. doi:10.2486/indhealth.33.67
- Kuempel ED, Stayner LT, Attfield MD, Buncher CR. Exposure-response analysis of mortality among coal miners in the United States. Am J Ind Med. 1995;28(2):167-184.
- Almberg KS, Halldin CN, Blackley DJ, Laney AS, Storey E, Rose CS, Go LHT, Cohen RA. Progressive Massive Fibrosis Resurgence Identified in U.S. Coal Miners Filing for Black Lung Benefits, 1970-2016. Ann Am Thorac Soc. Published online August 17, 2018. doi:10.1513/AnnalsATS.201804-261OC
- Blackley DJ, Halldin CN, Laney AS. Resurgence of a debilitating and entirely preventable respiratory disease among working coal miners. Am J Respir Crit Care Med. 2014;190(6):708-709.
- Blackley D, Crum J, Halldin C, Storey E, Laney A. Resurgence of Progressive Massive Fibrosis in Coal Miners — Eastern Kentucky, 2016. MMWR Morb Mortal Wkly Rep. 2016;65:1385-1389. doi:http://dx.doi.org/10.15585/mmwr.mm6549a1
- Doney BC, Blackley D, Hale JM, Halldin C, Kurth L, Syamlal G, Laney AS. Respirable coal mine dust in underground mines, United States, 1982-2017. Am J Ind Med. 2019;62(6):478-485. doi:10.1002/ajim.22974
Posted on by