Risk-Based Model to Resume Field Research and Public Health Service During the COVID-19 Pandemic
Posted on byDuring the COVID-19 pandemic, many workplaces across the world strictly limited or ceased in-person activities, including parts of the Federal government. While much work continued remotely, the National Institute for Occupational Safety and Health (NIOSH) needed to make decisions about allowing employees to travel to conduct workplace safety and health field research and public health service work. To assist with these decisions, NIOSH developed a risk-based model to conduct fieldwork, balancing the public health benefit of such work with the risks of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) exposure and transmission. The model is described in detail in a recent American Journal of Public Health article and can easily be adapted by other organizations for use in current and future situations.
In the initial phases of the pandemic, NIOSH developed and implemented a risk management decision tree (Figure 1) for work-related travel that considered four major determinants of risk of a NIOSH employee becoming infected with or transmitting SARS-CoV-2 while conducting field visits:
(1) site conditions and work requirements,
(2) level of COVID-19 community spread at the site and surrounding area,
(3) mode of transportation and length of stay, and
(4) controls in place.
Figure 1. Initial risk decision tree for NIOSH work-related travel
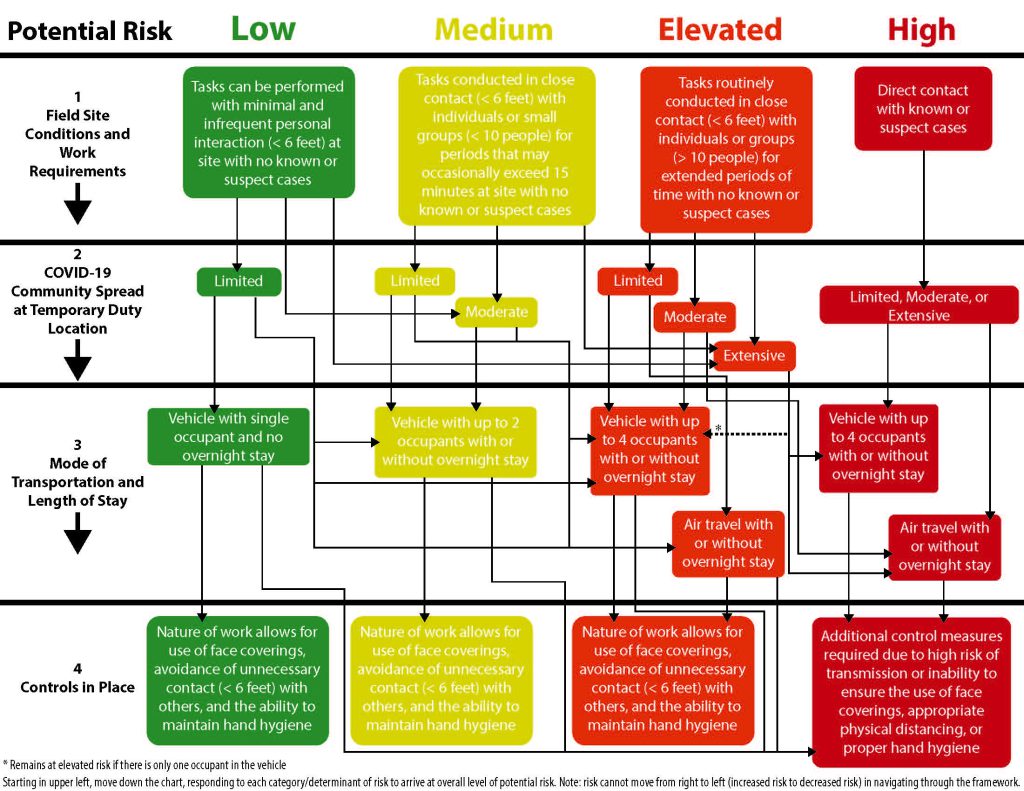
Prioritizing only the most urgent or time-sensitive field work, the initial decision tree facilitated the approval of 51 requests from NIOSH investigators for travel between October 2020 and July 2021.
Most of approved travel during the first year of the pandemic was determined to be medium or elevated risk. In one approved example, two research engineers were able to travel together in a car for four hours to conduct maintenance on a seismic monitoring station, necessary for researching and monitoring the impacts of seismic events in the mining industry, one of several industries that States identified as essential workers during the pandemic. Three of the approved travel requests were determined to be high risk with extensive COVID-19 transmission but involve an urgent public health need. In one such case, two investigators traveled to a worksite to investigate a suspected relationship between workers performing welding operations and developing a serious illness involving novel bacteria. Importantly, no COVID-19-related illness were reported from these work-related travel duties.
While successful in identifying high risk scenarios and permitting the continuation of limited mission-critical occupational health and safety research, the decision tree was somewhat complex and difficult to navigate. As the pandemic response progressed, so too did effective control measures, availability of vaccines, and improved access to data. Considering these improvements, an evaluation of the risk decision tree was conducted to overcome some of the observed complexities and integrate additional risk factors as appropriate. As a result of the evaluation, the risk decision tree was replaced with a relatively simple risk matrix framework (Figure 2) that was finalized in August 2021. This semi-quantitative model integrates county-level data on SARS-CoV-2 transmission with percentage of adult population fully vaccinated, two important determinants of risk of transmission, infection, and illness,[1] and characterizes varying levels of both metrics in terms of a travel location risk rating. The model also considers information on personal contact and mode of transportation in estimating a travel risk level. This matrix provided a more objective assessment of potential risk. Final decisions were made with additional consideration of the travelers’ vaccination status, any known control measures in place or to be implemented, and public health benefits of the proposed travel.
Figure 2. Simplified risk matrix and rating tool
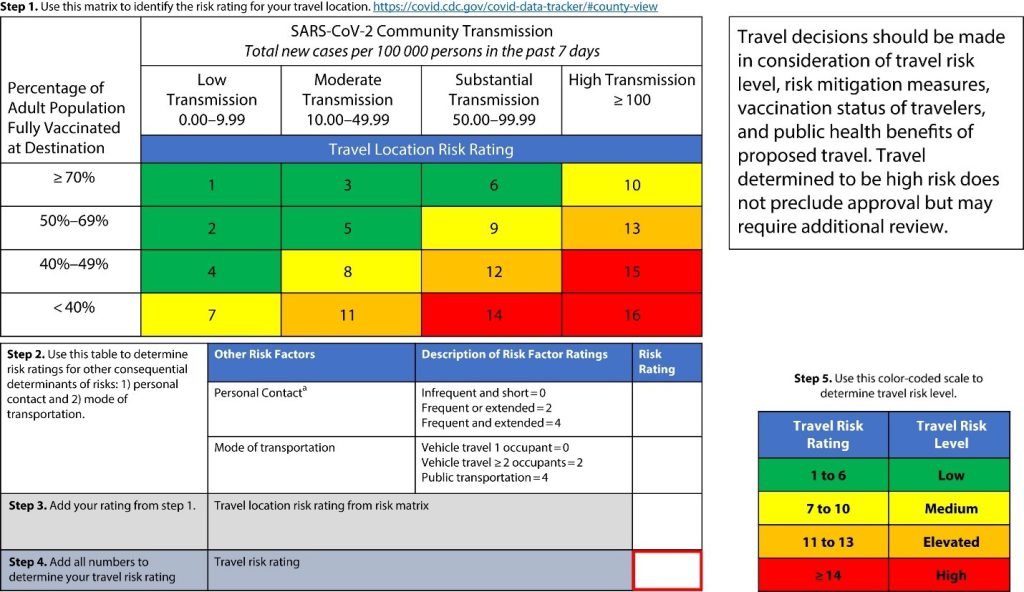
A risk matrix is just one of myriad tools that can be used in a larger risk assessment and management process. As noted in the article, the models implemented did have some limitations. Though considered in the travel approval process, the simplified risk matrix itself did not include risk factors (e.g., contact duration, personal risk factors for developing severe illness) that some would consider important for determining individual risk. Also, the cut points dividing potential levels of risk for each metric in both models were based largely on convenience rather than an in-depth analysis. However, with ongoing evaluation and review of data, the model is easily refined.
Presently, several attributes and methods of the risk matrix are reflected in the Centers for Disease Control and Prevention’s guidance related to COVID-19 community levels, most notably the use of a simple model that integrates a limited number of reliable COVID-19–related metrics to inform decision making at the community level.
These tools allowed NIOSH researchers to conduct limited mission-critical fieldwork while protecting field staff and workers during the COVID-19 pandemic. Delaying this critical work would have had real public health risks as NIOSH is the only federal institute mandated to conduct research and public health service work to prevent work-related injuries and illnesses.
Finally, the article notes how an approach like the described risk matrix may have wider applications when adopted and modified by those who are charged with managing any risk in their organizations. Organizations and their employees can benefit by developing and clearly communicating mitigation strategies in anticipation of changing risk to minimize potential disruptions to employees and work processes.
Please feel free to share or comment on how your organization prioritized travel or other necessary activities during the pandemic in order to meet critical needs while protecting your own staff.
Douglas Johns, PhD, MS, is Director of the NIOSH Spokane Mining Research Division.
Kristin Yeoman, MD, MPH, is a medical officer in the NIOSH Spokane Mining Research Division.
Joshua Harney, MS, is the Deputy Division Director of the Division of Field Studies and Engineering.
John Howard, MD, is the NIOSH Director.
Gerald Poplin, PhD, MS, is a Branch Chief in the NIOSH Spokane Mining Research Division.
[1] Centers for Disease Control and Prevention. SARS-CoV-2 infections and hospitalizations among persons aged ≥16 years, by vaccination status—Los Angeles County, California, May 1–July 25, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(34):1170–1176.https://doi.org/10.15585/mmwr.mm7034e5
Posted on by