Home Healthcare Workers: A Growing Workforce at High Risk for Workplace Violence
Posted on by
Home healthcare workers provide healthcare services to millions of Americans who need assistance at home. Home healthcare workers work closely with patients and often are in close contact with the public while they provide healthcare services to patients. Both situations can pose increased risks for exposure to workplace violence [1],[2].
The issue of violence in home healthcare will likely increase as the industry is projected to grow dramatically in the coming years. This growth may be impacted by shifts during the pandemic to telemedicine and in-home care. Substantial resources have been directed towards understanding, preventing, and managing workplace violence. Opportunities exist for a finer focus on modernized interventions that prevent workplace violence toward home healthcare workers and for fostering innovative solutions for addressing any resulting traumatic impacts.
What do home healthcare workers do?
Home healthcare workers deliver health services to patients in their homes. Personal care aides, home health aides, nursing assistants, and other care assistants are very important home healthcare workers who help clients with activities of daily living (e.g., bathing, dressing, and feeding), provide skilled nursing care including assistance with medication administration, and perform housekeeping chores [3],[4]. Requirements for formal training and certifications vary, depending not only on the state but also on the job and the health agency’s requirements. Other home healthcare workers are universally licensed and include nurses, therapists, and social workers who provide skilled nursing care, medical services and treatments, rehabilitation therapy, and social assistance [3].
The home healthcare workforce
Home health and personal care aides are some of the fastest-growing occupations, with a projected growth of 34% from 2019 to 2029; in 2019, the workforce numbered 3.5 million with a projected 1.1 million additional jobs through 2029 (BLS Occupational Outlook Handbook). In 2021, the American Staffing Association (ASA) reported that more than 74,000 home health and personal care aides are employed with ASA-affiliated home care agencies [5]. The projected growth is due to patients choosing to remain at home, increased prevalence of chronic illnesses, an aging population, and advances in medical technology that enable healthcare services to be delivered in patients’ homes. With this projected growth and the movement from hospital-based to home-based care, the risks for workplace violence and other safety concerns for home healthcare workers are expected to increase.
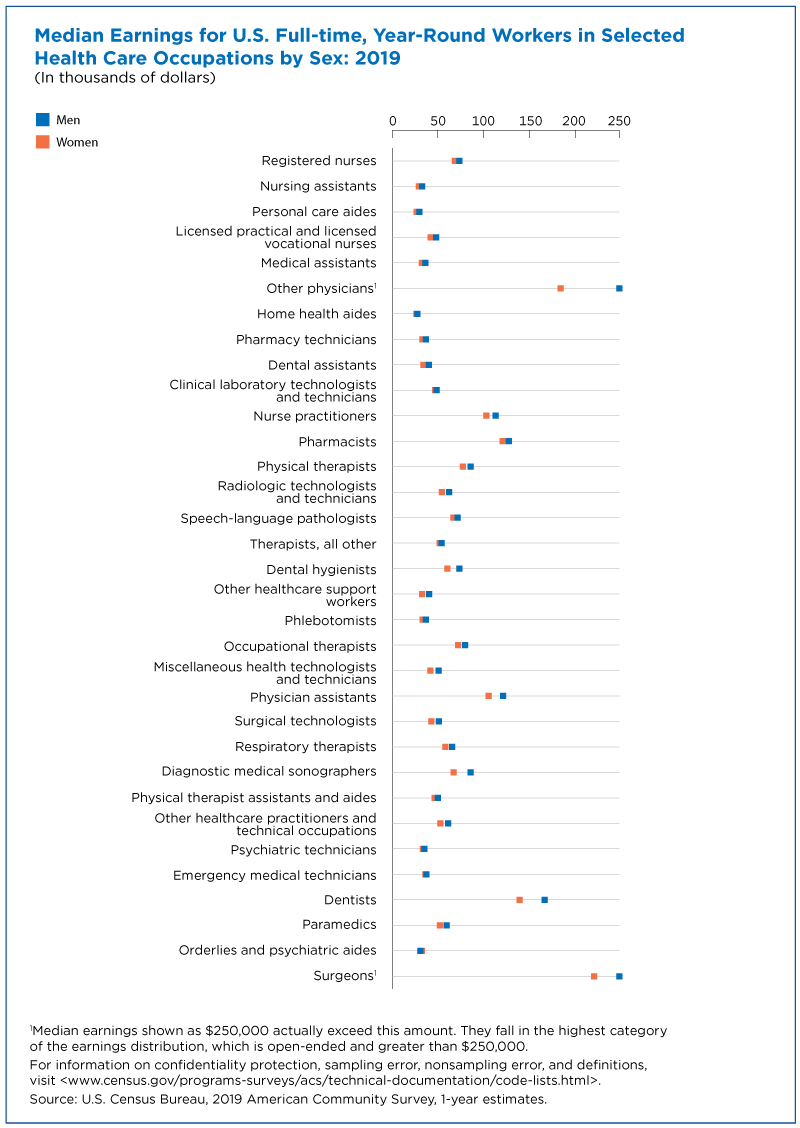
Home healthcare workers are largely female, non-white, and among the lowest paid in healthcare. In 2020, workers in the home healthcare services industry were reported to be 88% female, 29% Black or African American, and 19% Latino or Hispanic (BLS Current Population Survey [6]). The median annual pay for home health and personal care aides in 2020 was $27,080 annually and $13.02 hourly (BLS Occupational Outlook Handbook [7]). Home healthcare typically involves a nonstandard work arrangement (e.g., part-time, contingent, temporary, on-demand, and/or contract work). In some cases, home healthcare workers may not be entitled to minimum wage or overtime pay. These nonstandard work arrangements contribute to job insecurities and concerns of speaking up about working conditions and risks due to fear of job loss.
{kind=link}
Workplace violence definition and typology
Workplace violence is defined as the “act or threat of violence ranging from verbal abuse to physical assaults directed toward persons at work or on duty” [8]. Workplace violence is characterized by any work-related aggression or challenge to workers’ safety, health, or well-being from intimidation, abuse, or attack [9],[10]. The World Health Organization categorized workplace violence as physical, psychological (emotional), sexual, and racial [11]. Workplace violence includes acts of incivility, bullying, verbal abuse, physical assault, and sexual harassment.
To classify the relationships between the victim and the perpetrator, the workplace violence typology was developed [12]. A summary of the four types of workplace violence are: (1) Type I, criminal intent, an employee is robbed, or their property is vandalized; (2) Type II, a patient/client or family member attacks an employee; (3) Type III, a co-worker threatens or attacks another co-worker; and (4) Type IV, personal relationship, when someone known to the employee outside of work, such as a significant other, threatens or attacks the employee while at work.
Numerous and interrelated risks for workplace violence
Scientific studies have linked violence in home healthcare settings to negative emotional, cognitive, behavioral, physical, and psychosocial outcomes among workers. The adverse effects of violence can severely impact the delivery of healthcare services and the quality of care, and can result in diminished productivity, job dissatisfaction, drug and alcohol use, and poor health outcomes among workers [13]. Studies have presented several consequences of workplace violence in healthcare to include worker burnout, reduced quality of life, and mental health problems (such as emotional exhaustion, suicidal thoughts, depression, and anxiety) [14]. The job characteristics and requirements of home healthcare workers place them at high risk for workplace violence, particularly Type I and Type II. Home healthcare workers primarily work alone in situations that can be dangerous. In addition to workplace violence, they often face similar occupational hazards as other healthcare workers employed in hospital settings along with risks specific to the home care environment, such as unpredictability and decreased control of their work environment, lack of policies and procedures, and insufficient training [15-19].
Research studies have reported a range of 18% to 65% of home healthcare workers experiencing verbal abuse from patients [15],[17],[20-24]. As many as 41% of home healthcare workers have reported sexual harassment [15],[17]. Between 2.5% and 44% of home healthcare workers have reported being physically assaulted [15],[17],[23-25]. In one study, home healthcare registered nurses frequently reported demanding patients (34%), aggressive pets (27%), poor lighting in patient homes (21%), neighborhood violence/crime (19%), patients’ challenging family members (18%), personal security fears (14%), drug use in patient homes (13%), firearms in the home (9%), and racial/ethnic discrimination (8%) [20]. Researchers have also reported that physical or verbal threats of violence were associated with providing home care services to patients with a history of violence or patients with mental illness or substance use disorders [25].
Post-incident support and reporting systems
Post-incident support services can have great value for home healthcare workers’ well-being. Services might include peer support, formal debriefing, trauma-crisis counseling, and employee assistance programs. A study found post-incident support through debriefing increased workers’ awareness of workplace violence risks and also increased workplace violence reporting [26]. Reporting of workplace violence is very important to understanding the magnitude of workplace violence in the home healthcare industry and in providing data to inform future workplace violence prevention strategies [27]. Research into how to increase participation of home healthcare workers in post-incident debriefing is necessary to help prevent future events of workplace violence and improved worker health.
Preventing workplace violence to home healthcare workers
Different strategies can be used to protect home healthcare workers from violence. The issue is currently receiving attention in Congress [28]. Workplace violence in the home healthcare environment is complex and requires multi-faceted prevention efforts. One way to approach this is to apply Haddon’s Matrix to workplace violence in home healthcare (Table 1, adapted from McPhaul and Lipscomb [29]). The Haddon Matrix uses traditional public health terms such as ‘host’ and ‘agent/vehicle’ and applies them to the victim (in this case, the home healthcare worker) and the combination of the perpetrator (whose identity varies per the workplace violence type described above), their weapon, and the force of the assault, respectively.
| Table 1. An Application of the Haddon Matrix to Workplace Violence Prevention in the Home Health Workplace | ||||
| Phases | Home Healthcare
Worker (Host) |
Patient (Agent) | Physical Environment | Social Environment |
| Prior to Assault | Knowledge; Employer-provided self-efficacy training |
Employer should record and communicate any patient history of prior violence | Adequate lighting in the home
Assess potential and actual weapon presence Assess egress options. Request pets be confined |
Prior to visit, employer should clearly describe to patient the expectations for patient and family behavior.
Provide adequate resources to ensure safety Visit in pairs or with escort |
| During Assault | Verbal de-escalation
Escape techniques Personal alarms; Cell phones |
Increase distance between home healthcare worker and patient to reduce severity of injury | Readily available and known egress options
Active and accessible alarm systems |
Utilize duress code policies and security procedures |
| After Assault | Medical care; Crisis intervention counseling
Post-event debriefing Mandatory reporting of violent incidents |
Referral; Alternative care solutions
Law enforcement |
Evaluate role of and potential changes to physical environment
Update and maintain a list of identified environmental/com-munity risk factors |
All staff debrief with employer and identify relevant innovative prevention strategies |
As illustrated by the Haddon Matrix, there are a variety of steps that can be taken to prevent workplace violence to home healthcare workers before, during, and after acts of violence. Prevention is the primary responsibility of the employer; but, there are also roles and responsibilities for home healthcare workers, such as actively participating in training, following employer policies, reporting incidents to the employer, and participating in safety committees. Employers should adapt evidence-based prevention measures to prevent workplace violence among their home healthcare workers.
The following are examples of key prevention measures:
Provide standardized protocols that include:
- A zero-tolerance policy towards workplace violence
- Policies and rules on the safety of lone home healthcare workers in the field, such as regular cell phone contact or check-ins, and conducting home visits in pairs and/or with security escorts
- Rules and strategies related to visits in homes or neighborhoods where violence has occurred in the past
- Management commitment to home healthcare worker safety, including the formation and support of safety committees that involve field home healthcare worker participation and input
Provide comprehensive training to home healthcare workers on workplace violence that includes:
- Acquiring content specific to home healthcare workers and their work environment
- Assessing the work environment and surroundings for safety, including the presence of drugs of abuse, drug paraphernalia, weapons, and aggressive pets
- Recognizing signs of imminent violence, including verbal abuse and aggressive body language and/or posturing
- Employing verbal de-escalation techniques
- Utilizing escape and egress techniques
- Recognizing and reporting intimate partner violence and child abuse/neglect
Conduct post-visit assessments, recordkeeping, and evaluation. Employers work together collaboratively with home healthcare workers and safety committees to:
- Assess completed visits for violent events that occurred or were imminent (e.g., near misses)
- Identify factors that contributed to a violent event and/or hazardous environment
- Identify strategies and resources to prevent future occurrences
- Record events and monitor records for trends in workplace violence and the effectiveness of workplace violence prevention policies and practices
Concluding Thoughts
Home healthcare workers are a growing workforce who provide essential services in work environments that often have special challenges. Workplace violence may result in several adverse effects on home healthcare workers’ physical and psychological health. It is essential for home healthcare workers to be aware of risks of workplace violence in providing home care, and for employers to ensure that the work environment is safe. Evidence from scientific studies supports existing interventions for managing workplace violence in healthcare, particularly for home healthcare workers. Further research into improvement mechanisms and the efficacy of these interventions is needed to effectively address the risks of workplace violence to home healthcare workers.
The authors are members of the NORA Traumatic Injury Prevention Cross-Sector Council. Reducing violence in the workplace is one of the objectives in the NORA Traumatic Injury Prevention Research Agenda.
Tamara Felice Small, PhD, Supervisor, Home Healthcare at Complex Care Solutions
Susan Goodwin Gerberich, PhD, MSPH, Mayo Professor of Public Health Emerita; Inaugural Leon S. Robertson Professor in Injury Prevention; Former Director, Midwest Center for Occupational Health and Safety Education and Research Center, University of Minnesota
Anthony Oliveri, PhD, MPH, CIH, CSP, Assistant Professor, Division of Occupational and Environmental Medicine, Michigan State University (at the time the blog was written)
Christina Socias-Morales, DrPH, Research Epidemiologist, Division of Safety Research, NIOSH
Dawn Castillo, MPH, Director, Division of Safety Research, NIOSH
Richard Olawoyin, PhD, CSP, Associate Professor, Industrial and Systems Engineering Oakland University, Rochester Michigan
The authors thank fellow Council members who provided input and review on this blog:
Christine R. Schuler, PhD, Associate Director of Science, Division of Safety Research, NIOSH
John Swartos, ASP, Regional Safety Manager, Aerotek
Veronica Stanley, MSPH, CIH, CSP, CESCP, Adjunct Faculty, College of Safety and Emergency Service, Columbia Southern University
Related Resources
- Home Healthcare Workers: How to Prevent Violence on the Job
- Free On-Line Violence Prevention Training for Nurses
- The Unique Occupational Environment of the Home Healthcare Worker
- Nurses’ and Other Health Professionals’ Wellness and Safety Resource Update
- Violence in Healthcare
- Limiting Workplace Violence Associated with COVID-19 Prevention Policies in Retail and Services Businesses
References
[1] Kim, J. H., Lee, N., Kim, J. Y., Kim, S. J., Okechukwu, C., & Kim, S. S. (2019). Organizational response to workplace violence, and its association with depressive symptoms: A nationwide survey of 1966 Korean EMS providers. Journal of occupational health, 61(1), 101–109.
[2] Bloom, E. M. (2019). Horizontal violence among nurses: Experiences, responses, and job performance. Nurs Forum, 54(1), 77–83. https://doi.org/10.1111/nuf.12300 Epub 2018 Oct 17.
[3] Institute for Healthcare Improvement. (2018). No place like home: Advancing the safety of care in the home. March 9, 2021. Retrieved from
file:///C:/Users/15134/AppData/Local/Temp/No_Place_Like_Home_Advancing_Safety%20(1).pdf
[4] Paraprofessionals Healthcare Institute. (2019). U.S Homecare workers key facts. Accessed March 9, 2021. Retrieved from https://phinational.org/resource/u-s-home-care-workers-key-facts-2019/
[5] American Staffing Agency. (2021). Occupational Employment and Wage Statistics. Retrieved from americanstaffing.net
[6] U.S. Bureau of Labor Statistics, Labor Force Statistics from the Current Population Survey.
[7] U.S. Bureau of Labor Statistics, Occupational Outlook Handbook, Home Health Care and Personal Aides https://www.bls.gov/ooh/healthcare/home-health-aides-and-personal-care-aides.htm Accessed: May 5, 2021
[8] National Institute of Occupational Safety and Health. (2018). Occupational violence. Accessed March 9, 2021. Retrieved from https://www.cdc.gov/niosh/topics/violence/default.html
[9] Hoyle, L. P., Smith, E., Mahoney, C., & Kyle, R. G. (2018). Media depictions of “unacceptable” workplace violence toward nurses. Policy, Politics, & Nursing Practice, 19(3–4), 57–71.
[10] Shea, T., Sheehan, C., Donohue, R., Cooper, B., & De Cieri, H. (2017). Occupational violence and aggression experienced by nursing and caring professionals. Journal of nursing scholarship, 49(2), 236–243.
[11] World Health Organization (2021). Framework guidelines addressing workplace violence in the health sector. Retrieved June 28, 2021, from https://www.who.int/violence_injury_prevention/injury/work9/en/
[12] The University of Iowa Injury Prevention Research Center. (2001). Workplace violence: A report to the nation. Iowa City, IA: University of Iowa.
[13] Liang, Y., Wang, H., & Tao, X. (2015). Quality of life of young clinical doctors in public hospitals in China’s developed cities as measured by the Nottingham Health Profile (NHP). International journal for equity in health, 14(1), 85.
[14] de Looff, P., Nijman, H., Didden, R., & Embregts, P. (2018). Burnout symptoms in forensic psychiatric nurses and their associations with personality, emotional intelligence and client aggression: A cross‐sectional study. Journal of psychiatric and mental health nursing, 25(8), 506–516.
[15] Nakaishi, L., Moss, H, Weinstein, M., Perrin, N., Rose, L., & Anger, W. K. (2013). Exploring workplace violence among homecare workers in a consumer-driven home healthcare program. Workplace Health and Safety, 61(10), 441-450. doi:10.3928/216507991306101004
[16] National Institute of Occupational Safety and Health. (2012). Home healthcare workers. Accessed March 9, 2021. Retrieved from https://www.cdc.gov/niosh/docs/2012-118/pdfs/2012-118.pdf
[17] Hanson, C. G., Perrin, A. N., Moss, H., Laharnar, N. & Glass, N. (2015). Workplace violence against homecare workers and its relationship with workers health outcomes: A cross-sectional study. Public Health, 11, 2-13. doi:10.1186/s12889-014-1340-7
[18] Gross, N., Peek-Asa, C., Nocera, M., & Casteel, C. (2013). Workplace violence prevention policies in home health and hospice care agencies. The Online Journal of Issues in Nursing, 18(1). doi: 10.3912/OJIN.Vol18No01Man01
[19] Vladutiu, J. C, Casteel, C., Nocera, M., Harrison, R., & Peek-Asa, C. (2016). Characteristics of workplace violence prevention training and violent events among home health and hospice care providers. Journal of Industrial Medicine, 59, 23-30. doi:10.1002/ajim.22543
[20] Canton, N. A., Sherman, F. M, Magda, A. L., Westra, J. L., Pearson, M. J., & Raveis, H. V. (2009). Violence, job satisfaction, and employment intentions among home healthcare registered nurses. Home Care and Hospice Professional, 27(6), 364-373. doi:10.1097/01. NHH0000356828.27090.bd
[21] Geiger-Brown, J., Muntaner, C., McPhaul, K. M., Lipscomb, J. A., & Trinkoff, A. (2007). Abuse and violence during home care work as predictor of worker depression. Home Healthcare Services Quarterly, 26(1), 59-77. doi:10.1300/J027v26n01_05
[22] Karlsson, N. D., Markkanen, P. K., Kriebel, D., Gore, R. J., Galligan, C. J., Sama, S. R., & Quinn, M. M. (2019). Home care aides’ experiences of verbal abuse: A survey of characteristics and risk factors. Occupational Environmental Medicine,76 (448-454). doi:101136/oemed-2018-105604
[23] Quinn, M. M., Markkanen, K. P., Galligan, J. C., Sama, R. S., Kriebel, D. Gore, R. J. & Davis, L. (2016). Occupational health of home care aides: Results of the safe home care survey. Occupational and Environmental Medicine, 73(4), 237. doi:10.1136/oemed-2015-103031
[24] Sherman, F. M., Gershon, R. R., Samar, M. S., Pearson, M., J., Canton, N. A., & Damsky, R. M. (2008). Safety factors predictive of job satisfaction and job retention among home healthcare aides. Journal of Environmental and Occupational Medicine, 50(12), 1430-1441. doi:10.1097/JOM.0b013e31818a388e
[25] Byon, D. H., Storr, C., Edwards, L., & Lipscomb, J. (2016). Client history and violence on direct care workers in the home care setting. American Journal of Industrial Medicine, 59, 1130-1135. doi:10.1002/ajim.22652
[26] Arnetz, J. E., & Arnetz, B. B. (2000). Implementation and evaluation of a practical intervention programme for dealing with violence towards health care workers. Journal of Advanced Nursing, 31, 668–680.
[27] Hogarth, K. M., Beattie, J., & Morphet, J. (2016). Nurses’ attitudes towards the reporting of violence in the emergency department. Australasian Emergency Nursing Journal, 19, 75–81.
[28] H. R. 1195. Workplace Violence Prevention for Healthcare and Social Service Workers Act. Accessed June 10, 2021. Retrieved from https://www.congress.gov/bill/117th-congress/house-bill/1195
[29] McPhaul KM and Lipscomb JA. Workplace Violence in Health Care: Recognized but not Regulated Online J Issues Nurs. 2004 Sep 30;9(3):7. https://pubmed.ncbi.nlm.nih.gov/15482093/
Posted on by