
An Evaluation of “My Family Health Portrait”: Strengths and Opportunities
Posted on byCDC has hosted My Family Health Portrait (MFHP) since September 2018. Understanding current use of MFHP can help identify opportunities to improve and promote MFHP. We used Google Analytics to explore use of MFHP from Jan 1, 2019 to Dec 31, 2020. Google Analytics is a third-party tool that tracks user information, such as browser, language, screen resolution, and, in some cases, location, age, and gender.
Who are the users?
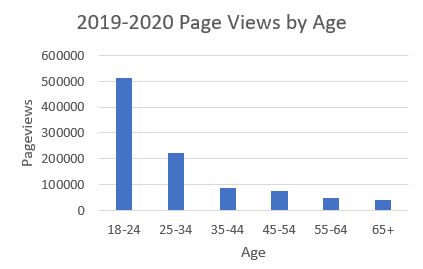
MFHP had more than 2.9 million page views from more than 400,000 sessions from 2019 to 2020. Google Analytics had demographic information for about 1/6 of these page views. Users tended to be younger (52% 18-24 years old), female (71%), and almost all from the United States.
How are users interacting with MFHP?
Page views peaked from January to February and from September to October and declined during the winter holidays and throughout the summer months. Other Public Health Genomics Knowledge Base pages and the CDC family health history portal main page show similar but weaker trends, with more daily or monthly variability. CDC and other federal agencies promote National Family History Day on Thanksgiving. Our analysis found a lower number of page views for the week of Thanksgiving, followed by a small peak in early December. Users typically only visited once and typically explored 14 pages. However, some users returned to MFHP for additional sessions, including few who returned more than 100 times. The median time per session was 31 seconds, which is not adequate time to fully utilize MFHP. Most users accessed MFHP from a desktop (92%), with the remainder using a mobile device (4.4%) or tablet (3.6%). While bounce and exit rates were similar between tablet and desktop users, mobile users had much higher bounce (59% vs 18%) and exit rates (21% vs 8%), which is not surprising as MFHP is not currently mobile friendly. In comparison, the mobile friendly CDC family health history portal had a higher percentage of mobile users (14.4%) but a lower percentage of tablet users (1.7%).
Where are users coming from?
Google Analytics could only identify how about 25% of users accessed the tool. Of these, most came from referral links on other websites, with a smaller portion originating from search engines, email, and social media (mainly Facebook).
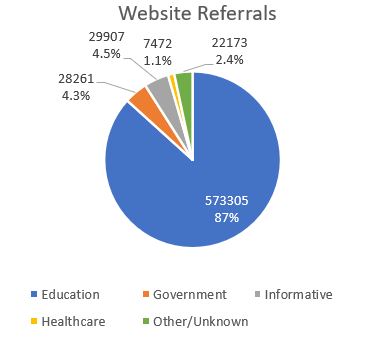
Among website referrals, about 87% originated from websites related to education, such as online classroom portals, indicating high awareness of the tool among educators. Government websites accounted for 4.3% of referrals including several NIH, NLM, and ODPH websites, which reflect the strong partnership with NIH, which originally hosted MFHP. Only five referrals came from state and regional health department websites, suggesting a need to expand partnerships at the state and local level. Other referrals came from health systems, insurance, patient advocacy, scientific society, scientific journal, and other websites.
Analysis Limitations
Our analysis had some important limitations, including the user data we could access. We only had information on users’ age and gender for 1/6 of page views and most referrals were “direct” and could not be tracked. We had to categorize some of the analysis by hand which can lead to bias. Google Analytics cannot identify whether users correctly filled out MFHP.
Recommendations
Based on this analysis, we propose the following to improve and promote the tool:
- Modify the MFHP to be more user friendly to older adults.
Increasing font size, using colors to aid navigation, and making error messages clear could make MFHP more friendly to older adults.
- Consider timing of MFHP promotional efforts.
Thanksgiving might not be the ideal time for promotion as it is a short holiday. CDC might extend heavy promotion into the winter holidays when families typically have more time off and gather together for longer periods of time. Communication efforts could also focus on times when usage was highest. For example, page views peaked in September, and promoting MFHP as a back-to-school activity to be completed each year might encourage repeat users.
- Leverage the existing educational referrals of MFHP by creating content for educators.
MFHP has been used in middle and high school, as well as genetic ethics, medical genetics, epidemiology, and nursing classes in college. Developing materials on MFHP for educators, such as slide sets and lesson plans, could further increase use in classroom settings.
- Increase referrals through engaging social media and email messages and search engine optimization.
Increasing engagement with social media followers and email subscribers might make them more likely to visit links such as those to MFHP. For example, social media messages could ask followers questions, and emails could share office updates. Applying search engine optimization best practices, including adjustments in the coding of the MFHP website, could increase the number of users reaching the site through search engines such as Google and Bing.
- Make MFHP easier to use to retain more users.
Lowering the reading level and simplifying the language could make MFHP more accessible to those with lower health literacy. Adding a short privacy statement, brief instructions, and background information to the landing page might help address user concerns and challenges. To assist with completion of the tool, users could be provided with resources about how to talk with family members about their family health history. Making MFHP mobile friendly would allow users to access the tool from any device, which would make engagement easier when families are gathered, and might encourage repeat visits.
Please share your experiences with MFHP and any suggestions for improvement in the comments section below.
Posted on by