In case you missed it: November HICPAC Public Meeting recap
Posted on by The Healthcare Infection Control Advisory Committee (HICPAC) held a public meeting Nov. 2-3, in Atlanta, Ga. Per the Federal Advisory Committee Act, and as has been done throughout the HICPAC meetings, official meeting minutes will be available on the HICPAC website in the coming weeks. Until then, below is a summary of key issues from the day’s discussion.
The Healthcare Infection Control Advisory Committee (HICPAC) held a public meeting Nov. 2-3, in Atlanta, Ga. Per the Federal Advisory Committee Act, and as has been done throughout the HICPAC meetings, official meeting minutes will be available on the HICPAC website in the coming weeks. Until then, below is a summary of key issues from the day’s discussion.
Key Moments
- On Day 1, the Isolation Precautions workgroup presented a draft of Part 1 of the new guideline.
- The committee discussed and debated needed revisions and heard public comments.
- On Day 2, the workgroup presented Part 1 draft revisions, which were informed by the Day 1 discussion and public comments. Changes were highlighted in the draft for easy viewing.
- The committee voted on whether the updated (revised) Part 1 draft presented on Day 2 could be sent to CDC for review before posting in the Federal Register. HICPAC met pursuant to the Federal Advisory Committee Act (Public Law 92-463). Part 1 cannot be considered final until posted in the Federal Register for public comment, revised for public comment, and presented and voted on again in 2024.
Watch recordings of the live public webcasts:
- Live Webcast on YouTube – Thursday, November 2, 2023
- Live Webcast on YouTube – Friday, November 3, 2023
Isolation Precautions Discussion & Vote
A large portion of the November meeting was dedicated to the presentation and discussion of the first section of the Isolation Precautions guideline update, titled the 2024 Guideline to Prevent Transmission of Pathogens in Healthcare Settings (Part 1). On Day 1, the workgroup presented detailed read-throughs of the new 24-page draft for committee review and consideration. The draft’s first section focuses on infection control concepts, including pathogen transmission pathways (how pathogens spread via the air and by touch) and type of personal protective equipment (PPE) available to healthcare workers.
The workgroup presented key updates to the 2007 guideline, including:
- Clearer and more concise language and formatting, to better align with adult learning principles. Instead of using roman numerals and long narratives, the workgroup suggested that the general needs for PPE and its value be described more plainly. Doing so would also make the section more usable to healthcare workers, reducing its length significantly from the current 207 pages, and avoiding repetition of content maintained in other guidelines.
- Using more protective practices and PPE to address new and emerging pathogens of concern. Among the proposed new categories for transmission-based precautions, Special Air Precautions recommends the use of NIOSH-approved® fit-tested N95 (or higher-level) respirators as the default option during care of patients with pandemic or emerging respiratory viruses. Other recommended categories to prevent transmission by air include Routine Air, which would have healthcare personnel wear a mask and eye precautions for endemic respiratory pathogens, and Extended Air Precautions, which would be used when providing care to patients with pathogens that can spread efficiently across long distances and over extended times. Detailed descriptions of these new categories can be found starting at line 441 of the draft Part 1.
- Updating the conceptual framework for respiratory pathogen transmission, including a continuum of pathogen transmission by air, rather than the dichotomy of “droplet” versus “airborne” transmission.
The workgroup did not make pathogen-specific recommendations for infection control. Drafting of that section will begin after Part 1 is completed, likely Spring 2024. Pathogen-specific recommendations will be reviewed and updated in segments based on pathogen types. Current pathogen-specific recommendations found in the 2007 Appendix A should continue to be used until recommendations for all pathogens are updated in the new Part 2.
On Day 2, the membership discussed the proposed draft of the first section. Members weighed questions such as the need to ensure availability of PPE in all healthcare settings, source control, the importance of describing the doffing technique, impact of ventilation methods, prevention considerations for transporters (people who help escort patients within a facility), and how to define “cohorting” and “patients” for different healthcare settings.
Input from both days of discussion were incorporated into a revised draft of Part 1. At the end of the meeting on Day 2, the membership took a vote to approve the updated draft for CDC review. HICPAC met pursuant to the Federal Advisory Committee Act (Public Law 92-463). The vote to send the draft to CDC for review and posting for public comment was passed; CDC program staff and leadership will review to determine if the draft should be returned to the workgroup for revisions or if it is ready for posting to the Federal Register. If the draft is approved for posting by CDC, it will be available on the Federal Register for 60 days for public review and comment. Learn more in a Q&A about the HICPAC guideline update process.
Other Discussions & Votes
On Day 1, the HICPAC members also heard proposed updates of patient placement and PPE recommendations for the Andes and Nipah viruses and an update from the Draft Infection Control in Healthcare Personnel Workgroup. The membership discussed the proposed drafts and voted on Day 1 to accept these drafts and send them to CDC for review.
Public Comment
HICPAC heard public comments on both days of the public meeting. Given the number of interested commenters, HICPAC used a lottery system to select and order public commenters. Those who were unable to present their comments were encouraged to provide written comments by 11:59 p.m. on Nov. 6. Oral and written comments submitted before the deadline will be included in the meeting minutes and will be posted to the HICPAC website. Read more information on the written comment process and deadline.
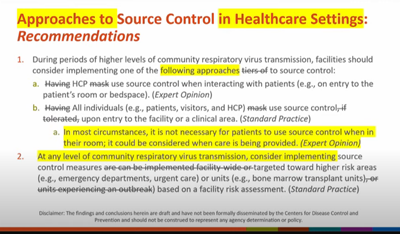
Public comments were considered in the edits to the working draft. For example, HICPAC specifically expanded considerations for use of source control, even beyond the current CDC recommendations for use when community respiratory virus transmission is high, in the Day 2 draft aligning with public commenter requests.
All attendees were encouraged to make official comments in the Federal Register when a draft passes voting, as part of the public comment period. The meeting convened with a summary of next steps. The committee will publish meeting minutes to the HICPAC website, and the draft guidelines will go to CDC for review and, if approved, then be posted to the Federal Register for comments on the draft.
Stay informed on HICPAC updates by signing up to receive e-mail alerts when new blogs post here. Search “Safe Healthcare Blog” on the CDC News & Updates Manage Subscriptions page. Additional information is also available on the HICPAC website.
Posted on by